> But pharma portfolios operate on the lognormal success model of VCs. Without the blockbusters, you can’t fund “development” of the failures that could lead to another blockbuster.
That was the point of my whole Humira example though: high pharmaceutical prices did not fund its development.
This assertion that drugs have to be expensive or they can't be developed keeps getting repeated, but there's little evidence to support it and even less evidence that they need to be this expensive. This argument is further troubled by little details like drugs being 600% more expensive in the US than in other countries, indicative of more of a "how much money can we extract from vulnerable people" strategy than a "how much will it cost to develop the next great drug" strategy.
To put this into perhaps more familiar terms, AbbVie's behavior is far closer to Intellectual Ventures than to Y Combinator, and yet people here keep defending it.
>Except the cost of many drugs continues to go up, even as they're commercially available and R&D has been recouped
A successful drug doesn't have to recoup its own R&D costs, it also has to recoup the costs of all the drugs that failed to make it to approval. It's not any different than VC investing. Just because one company in a portfolio returned 10x ROI, doesn't mean you can be like "alright guys, you made back all your money, now turn yourself into a non-profit".
>The R&D funding came from the previous drug, not the current drug.
In practice, yes that is often the case, but it doesn't matter for the new drug development decision.
If a new drug is unprofitable, it doesnt matter if there are funds from a prior one. A company will invest it elsewhere instead of spending it on a revenue negative drug.
Similarly, If a new drug looks profitable but internal funds are scarce, the Company will secure funding or sell distribution rights to raise the funds.
The Key role that the US is currently playing to making drugs profitable to develop that otherwise would not be.
I have worked on several programs, and the question is always "what is the return on investment" and never "how much do we have in the bank".
> "Why would we? Pricing shouldn't be a political decision. It should be a rational decision based on merits and values," he said. "Hundreds of millions of investor money has gone into the company, and if there is no return for those investments, there will be no new drugs because nobody's going to do that in the future, right?"
As terrible as it sounds, this logic seems sound to me. If we think having this type of drug is worth the > $100MM it took to develop, then health systems should either fund the $100MM research, or they should let private companies do it and pay them fairly for their work. $1MM for something so expensive to develop with so few possible users doesn't seem crazy to me.
If the $100MM is in fact not worth it, then, well, you get the situation we have now.
I'm sure a lot of people will read this article and think the owners/funders of the drugs are the bad guys. But nobody can be expected to work for free.
> Promotional spend has a positive ROI (or you wouldn’t do it).
That's incorrect; promotional spend on prescription drugs is the globally suboptimal result of a prisoner's dilemma where the prosecutors are going around saying "hey, that guy over there snitched, so should you". There is absolutely no guarantee that ROI is positive.
> Who do you think provides capital for drug development? The Grenadier Guards?
Most of basic drug development happens in labs e.g. at universities that are funded mainly by public sources.
Per the latest PhRMA member survey, drug companies spent about $13 billion per year on preclinical R&D, which was about 15% of their total R&D spend. Meanwhile the NIH alone provides about $40 billion per year for preclinical research. So funding for actually finding new drugs and therapies is dominated by other funding sources than drug companies.
If you look at e.g. Pfizer and J&J, more than 85% of their revenue comes from drugs that were invented elsewhere. Just to clarify, I'm not saying clinical trials isn't a necessary and expensive thing. But in large part it's not developing drugs, it's checking that there are no big side effects and that efficacy remains what you saw at small sample sizes.
For instance mRNA vaccines were invented in publically funded laboratories. Monoclonal antibodies that work against inflammation is another example. And of course CRISPR, which is very promising.
> The actual cost to develop a single successful drug, if you pass all the clinical trials, is in the ballpark of $500M or so.
I'd love to see a source for that.. Not even Pharma claims figures that high. Take Sofosbuvir for example; It was discovered in 2007, was developed through 2011 and then the company was acquired by Gilead while they had multiple Phase III trials running. In that time period, they spent a total of $230 million on R&D -- for all of their candidates. They also had two other compounds that were undergoing Phase II trials.
> The Phase III clinical trial by itself is well over $100M, much more if you're doing a large, long-term clinical study for a difficult problem (say, Alzheimer's or cancer).
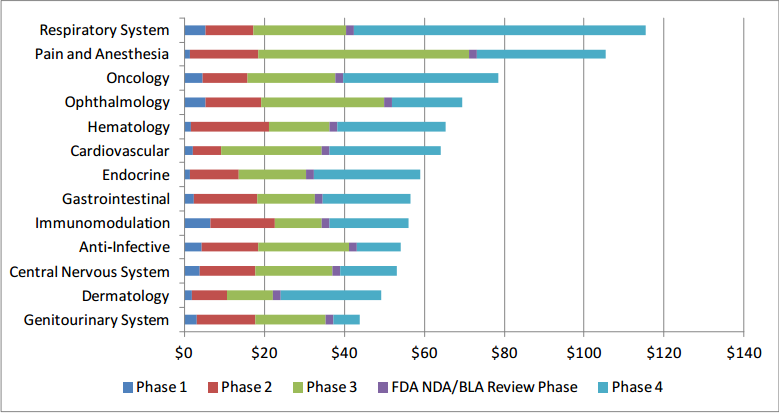
Nah. Not even close. HHS's most recent look placed Phase III at $19.9M, with very few classes of drugs costing more than $50M total for all phases (Ignoring IV since those are often more marketing than R&D)[1]:
> Something like 50% of all drugs fail in phase III.
The average is closer to 60% success rate, with some areas up to 75% success.[2] And it's not like if you fail the Phase III, the compound is scrapped and all of that work is wasted. There's an entire industry behind drug "repurposing, repositioning and rescue" to purchase and retarget promising compounds.
> But to be fair, the US pharma sector spends roughly as much on marketing as it does on R&D.
Spending money on marketing lowers prices by increasing volumes.
If you spend a billion dollars on R&D and then spend nothing on marketing and sell to 200,000 customers, they would each have to pay $5000 to fund the R&D. If you spend a billion dollars on R&D and two billion dollars on marketing and sell to a million customers, they would each have to pay $3000 to fund both the R&D and the marketing.
And it also does something useful, assuming the new drug is actually beneficial, by making people aware of the existence of something that would make their lives better. It helps no one to invent a great new thing that then nobody uses because nobody knows it exists.
> And a huge chunk of that R&D budget goes into analogue drugs to either sidestep patents from rivals or maintain profit margins when their own patents expire (they can then use that huge marketing budget to get the newly patented drug to take over for the old one with the nearly-expired patent, despite small or non-existent benefits from a medical perspective).
It doesn't actually cost that much to do that because you already know what you're looking for in that case. It's the real R&D that costs money.
> So long story short, there's a pretty good case to be made that public research with somewhere between 1/10th and 1/5th the budget of big pharma is all it takes to match or overtake them in innovation, as measured by actual benefit to the patients.
The biggest problem with public research funding is how to allocate it.
With a profit motive and market competition, the people who allocate research funding inefficiently go out of business and the people who allocate it well make a lot of money, and then have more money to fund more research.
Without that, research funding turns into defense contracting and then we waste trillions of dollars and have nothing to show for it. Or worse, politicians say we'll only need 1/10th of the budget even though the incentives aren't actually there to improve efficiency, and then we get 1/10th of the research.
> many critics of "Big Bad Pharma" who see the profitable drugs making it to market are unaware of the expensive failures that never make it that far.
But I think this image - that pharmaceutical companies are constantly risking their financial future pouring resources into research for new drugs which will finally cure some disease that has plagued humanity - is also a mischaracterization of reality.
For instance, drug companies also spend a large portion of their research budget developing "novel compounds" which are based on small chemical changes to existing drugs, just for the purpose of extending their patent and increasing the profitability (read: cost to consumer) of an existing treatment. So it's not as if all the resources they put in to research represent some altruistic good.
To be honest, I think the incentive structure for drug companies, like many things in healthcare, is just not ideal for producing the best outcomes. Their ideal business model is to own expensive drugs which sick people have to take for their entire lives. If they produce truly curative treatments, that's actually a net loss for them.
As some people have suggested, it would make a lot of sense to nationalize drug research in the US. The idea is you bring the top pharmaceutical researchers into the NIH, and while this would require a big up-front investment, you might even be able to operate at a profit by licensing the drugs they develop to the rest of the world.
Also, in a single-payer world, you would have the healthcare provider under the same financial umbrella as the people creating the drugs. As a result, the incentive would be to drive treatment costs down.
>> The true cost of bringing a drug to market is 2.8B
While it does makes sense that pharma r&d is expensive ,It's really hard to believe those numbers, specially that they always seem to change: first it was ~$700M/drug, than ~1.5B and now 2.8B ?
>There is a very lengthy process of getting drugs through the FDA which makes investment's return-on-investment difficult to justify without raising already available drug prices.
The lengthy process is there for a reason, it's not some hamper on profits just to hamper profits. Do we believe that the FDA is full of short sellers? Poor Pfizer, they won't get more money than they've spent! The logic here is sinister. ROI on drugs shouldn't be every dollar spent gets you a dollar ten and a drug, it should be you have a drug. The basic research that informs R&D spending has a ROI of zero by business metrics.
It is sad to think that the trajectory of medical advancement is dictated not by what we can achieve as scientists, but what is profitable for businessmen. When Jonas Salk was asked who owns the patent to the polio vaccine he developed, he replied, "Well, the people, I would say. There is no patent. Could you patent the sun?" In 1988 there were an estimated 350,000 cases of poliomyelitis worldwide, in 2018 there were 29 (1). The global initiative to eradicate the disease would not have been possible had the vaccination been for-profit.
> If you look R&D spending by pharma companies, the research part costs about 1/3rd. The development part is 2/3rds of the cost.
You left off the marketing expense:
"In 2012, the pharmaceutical industry spent more than $27 billion on drug promotion— more than $24 billion on marketing to physicians and over $3 billion on advertising to consumers (mainly through television commercials)."
> Take a look at the Nature article that traced who discovered new drugs over the past decade or so. Over 2/3 were NOT invented by gov't or non-profit funding.
But that doesn't mean government can't invent or fund drug discovery.
> Nope. Development costs $1B+ by itself, as you can see from my source or your link. Marketing spend is on top of the R&D cost.
Irrelevant. You said: "And expensive drugs are expensive primarily because it really does cost $1B+ to develop a new drug" [emphasis mine] and I demonstrated this to be untrue. The data shows that the primary cost is not in R&D.
It doesn't matter what you say about the necessity of that sales and marketing. I didn't comment on that. The primary cost is still not in R&D.
> Third, drugs only account for 40% of J&J sales--their scary marketing budget includes lots of advertising for non-pharmaceutical products.
This may be true and perhaps more data is needed, but I haven't seen any evidence that demonstrates unequivocally that the primary cost of drugs in the US is due to R&D.
> I think the answer is that drug development is the kind of process which public institutions are particularly ill suited to manage.
> A drug company is free to pursue and fund development of drugs based on merit alone.
What?
The argument that only they can provide what the public needs is just an excuse to avoid competition, as it is everytime you hear it being made in any industry: Municipal broadband is not able to fulfill the requirements of the fast-pacing telecommunications market so we should outlaw it and subsidize the private sector even more so you can finally have that 1MB dsl line you were due in 1999.
The Pharma industry has been "caught" many times preferring and in some cases preventing development of "cures" to instead sell long lasting treatments. Like most businesses, the only merit they care about is what makes them the most money, and there is nothing wrong with that, but let's not make them the gallant saviors of the masses when their evident greed becomes apparent every quarterly report and lobbying all over the world to avoid any form of competition is just the latest example of it.
> Empirically, about 90% of the compounds that start at that first level fail to make it to the last level
That would be an incredible rate of success, depending on what 'first level' means. If you mean "reached human clinical trials", maybe, but dunno.
> It also seems that academia is not any better than pharmaceuticals at either developing the first step or pushing something to the end.
"it also seems" lacks rigour, but let that pass for now.
If academia develops 85% of the drugs that are released (I'll try to find a source for that, it's from memory) then the vast majority of failure costs (85% of them) are soaked up by the taxpayer. The few that are bought up by the drugs companies, are then sold privately. Very profitable.
"According to BBC News, in 2013 pharmaceutical companies enjoyed higher average profit margins than carmakers, oil and gas companies and media companies. Only banks had a profit margin comparable to Big Pharma, but Pfizer’s 42% profit margin blew every other company out of the water, prompting even a member of its own industry to say, “I wouldn’t be able to justify [those types of margins].”
In 2013, five pharmaceutical companies exceeded 20% profit margins: Pfizer, Hoffman-LaRoche, AbbVie, GSK and Eli Lilly."
> But wait, these drugs won't even exist if they didn't charge as much.
Why they should not charge fairly? How much is as much?
On the issue of innovation, profit seekers does not have enough courage to do this. Board of big companies live quarter to quarter because their compensation is directy linked to stock value. It doesn't matter how much money they already have. Here is quote from the ted talk[1] linked below.
> In the drug industry, for example, 75% of the “radically innovative drugs” in the United States are researched in nationally funded laboratories. Whereas drug companies focus their efforts on “me-too” drugs — varieties of proven, profitable drugs — governments will take on potentially game-changing “new molecular priorities,” despite the risks involved.
>This makes central planning remarkably easy compared to typical consumer goods.
What if bureaucrats are much more risk averse than investors? We may end up with less drugs. The same things happens when taxpayers get too many stories of paying scientist salaries for things that fail. Letting investors and those more knowledgeable of markets and drugs might end up making drugs that wouldn't happen on taxpayer money only.
>all it would take to expand that program to include later-phase clinical trials would be increased funding.
[1] claims ~60 new drugs approved in 2018. [2] puts the cost of a new drug, plus post analysis, at $3B. This is already ~180B, perhaps not counting the ~80% of drugs that fail to make it to market. For scale, the entire NIH budget is ~12B; the money paid by the govt for drug research is a tiny part of the cost to get the drug to market, (otherwise more universities would start their own drug companies)
Raising another 180B from taxpayers is no small feat, and if that could be done, it's not clear this is the best space to spend it.
It may be much cheaper overall to let investors take the risks (and thus also get rewards).
>A nationalized pharmaceutical industry that provides drugs at cost seems like it would be a tremendous boon to our society
Agreed, assuming that it would truly cost less to do this. The govt is not terribly efficient at many things the market provides, from power to package delivery. The most cost efficient outcomes usually come from govt ensuring markets are competitive, then letting companies fight for sales, causing them to develop and fight over efficiency gains.
A better fight might be to find ways to make the current market more competitive while still delivering results.
These numbers certainly aren't risk-free. Even if the company has 10 billion in cash, how many potential research leads can they bring to market? Not many.
>I agree with your comment in general, but I would just underline that the discovery component of a drug is often not paid for by the eventual vendor of the drug, but is instead paid for by taxpayers, other granting agencies, and venture capitalists.
In the case of the taxpayers and grants, i think it is important to keep in mind that these are explicitly given without strings attached or rights reserved because society decided that we want to encourage private research. It is fair to argue that perhaps we should change the model moving forward, but I find it fairly offensive when folk claim a retroactive ownership on this basis.
>Thus the eventual vendor of a drug won't necessarily have 5000:1 odds, but instead will be able to review and purchase the most promising candidate drugs based on data generated by other companies.
I wholeheartedly agree. the long >5000:1 is at discovery, i.e. the basic research that is often publicly funded. Once drugs have gone through enough screening to be used, the probability of approval is up to about 10:1 [1]. A lot of the bigger sales take place between phase 1 and 2, which probability of approval is up to perhaps 25%. Research institutions and early developers get paid based on the potential value and risk, and are not taken advantage of. The fact that companies often outsource early develop doesn't invalidate the their claim to their profits.
>The expensive part of bringing new drugs to market is testing in humans. Perhaps the US could bear some of these costs while, in exchange, shortening or eliminating patent protections.
This is an interesting idea. Two additional options that you may want to consider that wouldn't stifle development are expedited approval and government manufacture of generics. Due to the time value of money, faster approval increases the profitability of new drug development and without increasing prices to consumers. For generics, drug profits after loss of exclusivity are so far out that they don't significantly weigh in on the decision to develop a product or not.
> Academia should be the primary means of drug discovery. Drug manufacturing and distribution _should_ be a commodity business
As mentioned below, the discovery is not the biggest driver of costs.
But you should also ask yourself: why is this not already the case? Currently, there's nothing stopping other countries from using taxpayer money to fund drug development locally. Except, by and large, they don't - as mentioned in the article, most of the drug development that happens worldwide is funded by the United States, even for companies that are headquartered in Europe.
The answer isn't that those countries aren't interested in consuming the benefits of that research, because they are more than willing to purchase those drugs that were developed in the US at lower prices. The answer is that they just choose not to fund the research, either because it's too expensive to conduct clinical trials with taxpayer money, or because it's more effective to have that funded by the market, especially when that market is US patients, rather than European taxpayers.
{kind=link}
That was the point of my whole Humira example though: high pharmaceutical prices did not fund its development.
This assertion that drugs have to be expensive or they can't be developed keeps getting repeated, but there's little evidence to support it and even less evidence that they need to be this expensive. This argument is further troubled by little details like drugs being 600% more expensive in the US than in other countries, indicative of more of a "how much money can we extract from vulnerable people" strategy than a "how much will it cost to develop the next great drug" strategy.
For extra credit, take a look at AbbVie's notable products (https://www.drugwatch.com/manufacturers/abbvie/#abbvie-produ...) and see if you can identify any that they developed, or that they funded the development of.
To put this into perhaps more familiar terms, AbbVie's behavior is far closer to Intellectual Ventures than to Y Combinator, and yet people here keep defending it.
reply